



Insoles are among the most widely used foot health interventions worldwide. From everyday comfort to complex biomechanical correction, they play a vital role in managing pain and improving function.
This clinical guide presents 101 evidence-informed facts to help clinicians and informed consumers understand how insoles work and why they matter.
Definition
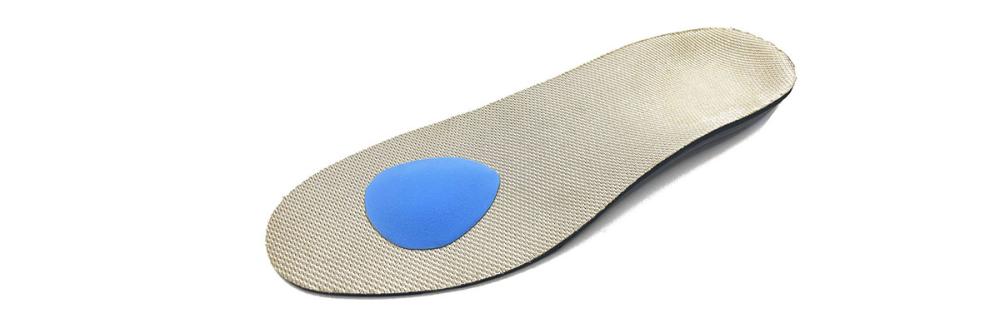
Insoles - also known as foot orthoses or shoe inserts - are removable devices placed inside footwear to redistribute pressure, improve alignment, enhance comfort and influence lower limb biomechanics.
How Insoles Work - And Why They Matter
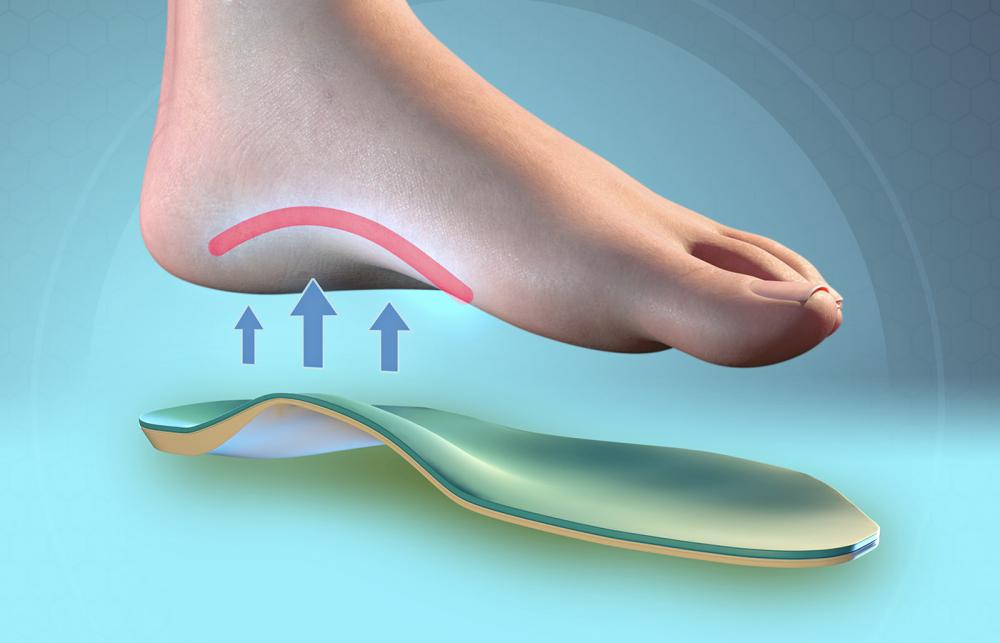
Insoles influence the interaction between the foot and the ground. By modifying load distribution, controlling motion, and enhancing shock absorption, they can reduce tissue stress and support optimal movement patterns.
They matter because foot dysfunction contributes to conditions such as plantar fasciitis, metatarsalgia, knee osteoarthritis, and lower back pain. According to research published in Journal of Foot and Ankle Research, orthoses can significantly reduce plantar pressure and pain in specific patient groups (https://jfootankleres.biomedcentral.com/articles/10.1186/1757-1146-6-25).
For further reading, see our guides on Plantar Fasciitis Treatment and What Are Orthotics?.
101 Facts About Insoles
Fundamentals
- Insoles date back to ancient civilisations.
- The term orthosis means to straighten or correct.
- Insoles can be prefabricated or custom-made.
- Not all insoles are medical devices.
- Foot orthoses are evidence-supported for heel pain.
- Comfort improves adherence.
- Material density affects function.
- Arch height varies between individuals.
- Foot posture changes with age.
- Weight and activity level influence prescription.
Biomechanics
- Insoles redistribute plantar pressure.
- They can reduce peak heel loading.
- They influence subtalar joint motion.
- Medial wedges alter pronation moments.
- Lateral wedges may benefit medial knee OA.
- Metatarsal pads reduce forefoot pressure.
- Heel cups increase rearfoot stability.
- Shock absorption reduces impact forces.
- Balance can improve with sensory feedback.
- Alignment influences proximal joints.
Materials
- EVA is widely used.
- PU offers durability.
- Carbon fibre increases stiffness.
- Silicone enhances cushioning.
- Cork provides natural resilience.
- Foams vary in Shore hardness.
- Top covers improve hygiene.
- Antimicrobial layers reduce odour.
- Heat-mouldable materials allow adjustment.
- Rigid shells provide control.
Clinical Applications
- Plantar fasciitis management.
- Flat foot support.
- High arch pressure redistribution.
- Diabetic ulcer prevention.
- Metatarsalgia relief.
- Achilles tendon load reduction.
- Shin splints management.
- Knee osteoarthritis offloading.
- Sports injury prevention.
- Paediatric gait support.
Fit and Prescription
- Shoe fit matters as much as the insole.
- Assessment should be holistic.
- Gait analysis improves accuracy.
- Gradual wear-in is recommended.
- Overcorrection can cause discomfort.
- Review is essential after issue.
- Custom devices require casting or scanning.
- 3D scanning increases precision.
- Trimming may be required.
- Education improves outcomes.
Comfort and Compliance
- Perceived comfort predicts success.
- Breathability enhances usability.
- Lightweight designs increase acceptance.
- Bulk reduces footwear options.
- Colour rarely affects clinical outcome.
- Texture influences sensory feedback.
- Moisture management prevents skin issues.
- Regular replacement is necessary.
- Wear patterns reveal gait habits.
- User feedback informs modification.
Risks and Considerations
- Improper fit can worsen symptoms.
- Diabetic patients require specialist advice.
- Children outgrow orthoses quickly.
- Not all pain originates in the foot.
- Footwear choice may limit effectiveness.
- Rigid devices may feel intrusive.
- Gradual adaptation reduces irritation.
- Allergies to materials are possible.
- Cost varies widely.
- Evidence quality differs by condition.
Performance and Sport
- Runners often use insoles.
- Shock attenuation may reduce fatigue.
- Stability features vary by sport.
- Studded boots need slim profiles.
- Cycling orthoses differ from walking types.
- Ski boots require specialist fitting.
- Elite athletes use custom solutions.
- Pressure mapping informs design.
- Energy return materials are emerging.
- Comfort enhances performance consistency.
Innovation and Future Trends
- 3D printing is expanding.
- Smart insoles track gait data.
- Pressure sensors monitor load.
- AI-assisted design is growing.
- Sustainable materials are developing.
- Recyclable foams are emerging.
- Modular systems allow adjustment.
- Cloud-based gait analysis exists.
- Telehealth assessments are increasing.
- Customisation is becoming faster.
Practical Insights
- Break-in periods vary.
- Replace every 6 to 12 months.
- Sports use accelerates wear.
- Children require regular review.
- Older adults benefit from cushioning.
- Arch support is not one-size-fits-all.
- Minimalist shoes change orthotic needs.
- Some conditions resolve without orthoses.
- Education reduces unrealistic expectations.
- Clinical follow-up improves outcomes.
- The right insole is individual.
Comparison Table - Prefabricated vs Custom Insoles
| Feature | Prefabricated Insoles | Custom Insoles |
|---|---|---|
| Cost | Lower | Higher |
| Manufacturing | Mass produced | Individually made |
| Fit precision | Standard sizes | Foot-specific |
| Clinical complexity | Mild to moderate | Moderate to complex |
| Adjustment | Limited | Highly modifiable |
Step-by-Step Guide - Choosing the Right Insole
- Identify symptoms and duration.
- Assess footwear type.
- Consider activity level.
- Start with evidence-based solutions.
- Trial prefabricated if appropriate.
- Seek professional assessment for persistent pain.
- Allow gradual adaptation.
- Review at 4 to 6 weeks.
How Insoles Influence Load
What Users Say
Patients commonly report reduced heel pain within weeks when compliance is high. Athletes note improved comfort over long distances. Clinicians emphasise that success depends on correct assessment rather than product cost.
Frequently Asked Questions
1. Are insoles the same as orthotics?
All orthotics are insoles but not all insoles are medical orthotics.
2. Do insoles weaken feet?
Current evidence does not support this claim when appropriately prescribed.
3. How long do insoles last?
Typically 6 to 12 months depending on use.
4. Can insoles cure plantar fasciitis?
They manage load but should form part of a broader treatment plan.
5. Are custom insoles always better?
Not necessarily. Research shows prefabricated devices can be equally effective for some conditions (https://pubmed.ncbi.nlm.nih.gov/15377904/).
6. Should children wear insoles?
Only when clinically indicated.
7. Do insoles help knee pain?
Lateral wedge insoles may reduce medial knee loading in osteoarthritis (https://arthritis-research.biomedcentral.com/articles/10.1186/ar4072).
References and Research Sources
- Landorf KB et al. Effectiveness of foot orthoses to treat plantar fasciitis. PubMed
- Journal of Foot and Ankle Research - Plantar pressure redistribution. View Study
- Arthritis Research UK - Lateral wedge insoles and knee OA. View Study
Author
Marc Cameron
Product Director, Algeos
Marc Cameron has over 20 years’ experience in foot health, orthotic materials and clinical supply. He works closely with podiatrists, physiotherapists, and orthotists across the UK and internationally to improve lower limb care through education and innovation.










Sold: Sold per Pair
Incl. VAT Exl. VAT