



A clinical guide for clinicians and informed consumers
Heel lifts are simple inserts that sit under the heel inside the shoe. Used well they can reduce painful tendon load in Achilles tendinopathy and buy time for strengthening to do its work.
This guide explains what heel lifts are, how they help, what patients report, how to use them step by step, and where they sit alongside other care.

How heel lifts work - why that matters
Biomechanical effects
- Elevating the heel reduces ankle dorsiflexion during stance which can reduce Achilles tendon strain and tensile load during walking JOSPT 2016 biomechanical study
- In a controlled lab study a 12 mm lift lowered indices of tendon loading while walking and running which supports its use when the goal is to temporarily offload the tendon BJSM lab report.
- Insertional cases experience both tensile and compressive loads. Lifts help by limiting end-range dorsiflexion which may reduce compression at the calcaneal insertion during gait and hill running Physiotherapy guideline review.
Clinical signal
- In a randomised trial of people with mid-portion tendinopathy heel lifts produced greater 12 week improvements in pain and function than eccentric exercise alone although both groups improved BJSM 2021 RCT. :contentReference[oaicite:3]{index=3}
- A 2024 protocol for the LIFT trial is evaluating heel lifts against a sham lift to quantify effect sizes and mechanisms in mid-portion cases which will clarify indications and dosing Trials 2024. :contentReference[oaicite:4]{index=4}
- For insertional tendinopathy a feasibility RCT showed a full trial is practical and safe which is a useful step toward higher certainty Journal of Foot and Ankle Research 2024 feasibility RCT. :contentReference[oaicite:5]{index=5}
- Recent work in insertional tendinopathy supports rehabilitation that reduces tendon compression by limiting dorsiflexion and it explicitly includes heel lifts as an element of care BJSM 2025 RCT discussion.
Clinical guidelines remain cautious where evidence is mixed. The 2018 revision of the JOSPT Achilles tendinopathy guideline did not make a firm recommendation for heel lifts while recognising their potential role which highlights the need to apply them within a broader programme JOSPT CPG 2018 and NICE CKS.
What users say
The following themes echo clinic feedback and the short-term insertional case series.
- Morning steps and first few minutes after sitting often feel easier with lifts in place which can improve day to day tolerance case series in insertional tendinopathy. :contentReference[oaicite:8]{index=8}
- Wearing lifts throughout the workday reduces low grade background pain enough to complete a strengthening plan more consistently biomechanical rationale. :contentReference[oaicite:9]{index=9}
- Some report calf tightness or a sense of forefoot pressure in higher lifts which usually settles with minor adjustments in height or footwear. Monitoring is still important.
Step-by-step guide to using heel lifts
- Confirm the diagnosis and location
Identify mid-portion versus insertional. Palpation site, symptom behaviour and loading history guide this. Consider imaging only when differential diagnosis is unclear or progress stalls. See NICE CKS for red flags and conservative care framing NICE CKS. - Pick a starting height
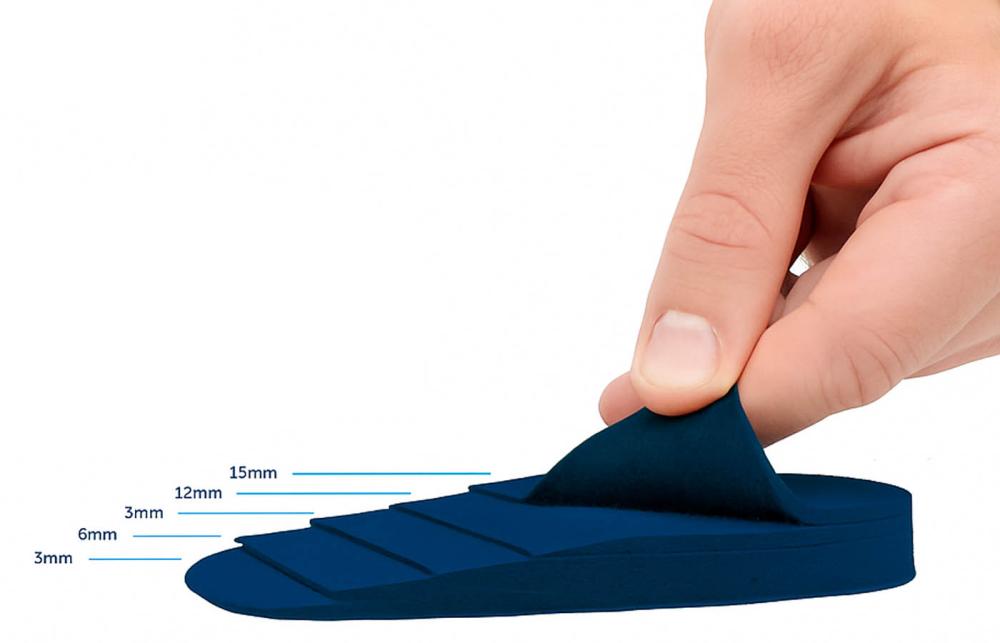
Most trials and lab studies use around 10 to 12 mm. Begin near this range if shoe volume allows then adjust to comfort and symptom response BJSM 2021 RCT and JOSPT 2016. - Fit both shoes and secure the heel
Use bilateral lifts to avoid a functional leg length change. Ensure the heel counter grips well to prevent slippage which can irritate insertional symptoms. - Match use to the diagnosis
Mid-portion: wear during most weight bearing hours while progressing calf strengthening. Insertional: combine with exercises that avoid deep dorsiflexion such as flat ground heel raises early on then gradually reintroduce range as tolerance improves BJSM 2025. - Integrate with progressive loading
Exercise remains the centre of care. Use a staged plan that moves from isometric to isotonic to energy storage and release to sport specific activity. This structure is supported in both mid-portion and insertional protocols BJSM 2025 RCT. - Review at 2 to 4 weeks
Track pain with activity, morning stiffness, VISA-A score where available and functional markers like single leg heel raises. Tweak height up or down by 3 to 5 mm if needed. - Plan to wean
As symptoms stabilise and strength improves reduce height gradually over 2 to 6 weeks. The goal is normal mechanics without the insert when feasible. If pain returns step back and progress slower. - Escalate if progress stalls
If there is minimal change by 8 to 12 weeks despite adherence consider imaging, footwear review, shockwave in selected cases, or referral. Align with local guidelines and patient goals Dutch multidisciplinary guideline.
Where heel lifts fit among other options
| Intervention | How it helps | Evidence snapshot | Strengths | Trade-offs | Typical use |
|---|---|---|---|---|---|
| Heel lifts | Reduce dorsiflexion and tendon strain which can lower pain during stance | Biomechanics support offloading. Mid-portion RCT shows benefit versus eccentric exercise at 12 weeks. More sham-controlled data emerging BJSM 2021 and Trials 2024. | Immediate symptom relief for many and easy adherence | May shift load to forefoot and can mask low capacity if used alone | Adjunct to exercise early then wean |
| Progressive calf loading | Builds tendon capacity and restores function | Cornerstone across guidelines and trials. Structure from isometric to sport specific is well supported BJSM 2025. | Drives long term change | Needs consistency and good coaching | Daily to near daily dosing with gradual progression |
| Load management | Reduces provocative volume or intensity while tissue adapts | Consensus across NICE CKS and multidisciplinary guidelines NICE CKS and Dutch guideline. | Low cost and individually tailored | May constrain training in the short term | Applied across the rehab timeline |
| Shockwave therapy | Non-invasive pain modulation to assist loading programmes | Mixed evidence and usually adjunctive within protocols. Consult local guidance | Useful when pain blocks exercise | Response varies and availability differs | Short courses alongside exercise |
Pictured: Heel Assist Heel lift
FAQ
What height is appropriate
About 10 to 12 mm is a practical starting point based on trials and lab work. Choose the lowest height that gives meaningful symptom relief without shoe fit issues BJSM 2021 and JOSPT 2016.
How long should I wear them
Most use them for the majority of weight bearing hours over 8 to 12 weeks while capacity is rebuilt through exercise then taper as tolerated. Trials often use a 12 week primary end point Trials 2024.
Do lifts help insertional Achilles tendinopathy
They can assist by limiting compressive load at end range dorsiflexion. Combine with exercises that avoid deep dorsiflexion early. Feasibility and early evidence support this approach while larger RCTs mature feasibility RCT and BJSM 2025.
Can heel lifts replace exercise
No. They are an adjunct that can make movement tolerable so that loading plans can progress. Long term outcomes depend on restoring tendon capacity through progressive loading. This is reflected across guidelines and trials Dutch guideline.
What are common pitfalls
Using only lifts without strengthening. Choosing a lift that is too high for the shoe which increases forefoot pressure. Wearing on one side only which creates a tilt. Not planning to wean once symptoms settle.
What should clinicians monitor
Pain during and after activity, morning stiffness, VISA-A or similar outcome measure, single leg heel raise capacity, walking or running tolerance. Adjust height and exercise stage based on these markers.
References and research sources
- Rabusin CL et al. Efficacy of heel lifts versus calf muscle eccentric exercise for mid-portion Achilles tendinopathy. Br J Sports Med. 2021 55(9):486-492. Link.
- Farris DJ et al. The effect of an in-shoe orthotic heel lift on loading of the Achilles tendon during shod walking. J Orthop Sports Phys Ther. 2016. PDF.
- Bourke J et al. Efficacy of heel lifts for mid-portion Achilles tendinopathy the LIFT trial protocol. Trials. 2024. Open access. :contentReference[oaicite:24]{index=24}
- Bourke J et al. Efficacy of heel lifts for insertional Achilles tendinopathy LIFTIT feasibility RCT. J Foot Ankle Res. 2024. Publisher PDF.
- Pringels L et al. Effectiveness of reducing tendon compression in the rehabilitation of insertional Achilles tendinopathy. Br J Sports Med. 2025. Article and PDF.
- Martin RL et al. Achilles pain, stiffness and muscle power deficits: midportion Achilles tendinopathy revision 2018. J Orthop Sports Phys Ther. 2018. PDF.
- NICE Clinical Knowledge Summary. Achilles tendinopathy management. 2025 access. Web.
- van der Vlist AC et al. Dutch multidisciplinary guideline on Achilles tendinopathy. Br J Sports Med. 2021. Open
- Nee RJ et al. Immediate and short-term effects of in-shoe heel-lift orthoses on insertional Achilles tendinopathy. Orthopaedic Journal of Sports Medicine. 2024. PDF.
Links were checked at publication. If a paywall appears try the PDF or institutional access.
Algeos Heel Lifts range can be viewed in our store.






Sold: Single lift
Incl. VAT Exl. VAT