



Article revised and updated April 2026
How to Reduce Heel Pain and Support Recovery
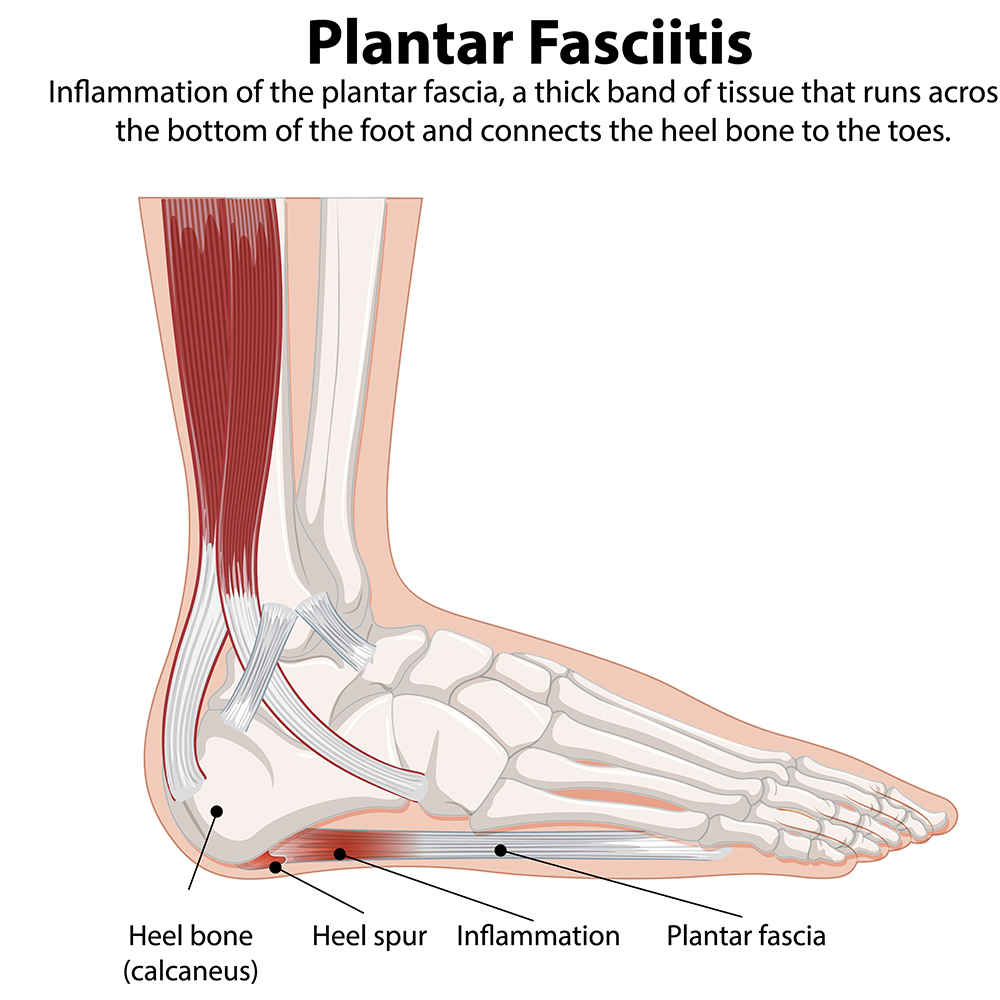
Plantar fasciitis is one of the most common causes of heel pain. It usually improves with a combination of stretching, supportive footwear, orthotic insoles, activity adjustment and time. More persistent cases may benefit from night splints, physical therapy or other clinician-led treatments.
Plantar fasciitis is one of those conditions that sounds oddly harmless until you actually have it. Then suddenly the first few steps in the morning feel like your heel has been personally insulted overnight. It is a very common source of heel pain, especially in people who spend long hours standing, walk on hard surfaces, run regularly, or wear unsupportive footwear.
The condition affects the plantar fascia, the thick band of tissue that runs along the sole of the foot from the heel toward the toes. When that tissue becomes irritated or overloaded, pain often develops around the heel or arch, particularly first thing in the morning or after sitting still for a while. UK and evidence-led guidance consistently points to self-management, stretching, supportive shoes and orthoses as key early treatments, with further options considered if symptoms drag on.
What Is Plantar Fasciitis?
Definition: Plantar fasciitis is pain and irritation involving the plantar fascia, usually felt under the heel and sometimes into the arch. It is commonly linked to repeated strain, overload, tight calf muscles, prolonged standing, running, weight gain, poor footwear, flat feet or high arches.
Plantar fasciitis is often described as a sharp or stabbing pain under the heel, particularly with the first steps in the morning. Some people also notice it after getting up from a desk, driving, or sitting on the sofa long enough to forget they own feet. The tissue may ease a little as you move, then flare again later after long periods of standing or walking.
Risk factors commonly include prolonged standing, reduced ankle flexibility, training overload, high-impact sport, higher body weight, flat feet, high arches and shoes that do very little to support the foot. NICE-backed UK guidance highlights self-care, appropriate footwear and activity modification as standard first-line measures.
Common Symptoms of Plantar Fasciitis
- Sharp heel pain when taking the first steps in the morning
- Pain after rest or inactivity
- Ache or tenderness under the heel or into the arch
- Symptoms that worsen after long periods on your feet
- Discomfort after walking barefoot on hard floors
- Tightness in the calf or Achilles area
If heel pain is severe, worsening, associated with trauma, numbness, major swelling or redness, or is not improving over time, it is worth getting assessed rather than assuming it is “just plantar fasciitis”.
What Causes Plantar Fasciitis?
Plantar fasciitis tends to build up rather than arrive out of nowhere. The fascia is under repeated mechanical stress with every step, especially if the foot is poorly supported or the tissues are tight and overloaded. Common contributing factors include:
- Long periods standing: especially on hard floors in healthcare, retail, salon, warehouse or factory roles.
- Training overload: a sudden increase in running, walking or impact exercise.
- Tight calf muscles: reduced ankle mobility can increase strain on the plantar fascia.
- Flat feet or high arches: both can alter how pressure is distributed through the foot.
- Poor footwear: thin, unsupportive or worn-out shoes can make symptoms worse.
- Higher body weight: extra load through the foot can aggravate symptoms.
Best First-Line Treatments for Plantar Fasciitis
The good news is that most cases improve with conservative management. Best-practice guidance supports a stepped approach that begins with simple, practical measures before moving on to more advanced treatments. Stretching, taping, education, load management and supportive footwear are widely recommended early on.
| Treatment | Why It Helps |
|---|---|
| Stretching | Improves flexibility in the calf and plantar fascia, helping reduce tension during walking. |
| Supportive footwear | Helps reduce repeated strain from thin or unstable shoes. |
| Orthotic insoles | Can support the arch, cushion impact and improve pressure distribution. |
| Activity modification | Reduces overload while allowing symptoms to settle. |
| Night splints | May reduce morning pain by keeping the fascia and calf on a gentle stretch overnight. |
| Manual therapy / physio | Can improve mobility, tissue tolerance and exercise progression. |
Stretching and Strengthening Exercises
Stretching is one of the most consistently recommended self-care strategies for plantar heel pain. NHS patient guidance specifically includes calf and plantar fascia stretching, and broader best-practice evidence supports exercise as part of early management.
Useful exercises include:
- Calf stretch against a wall: Keep the back heel flat and the knee straight to stretch the calf muscles.
- Towel stretch: Sit with your leg extended, loop a towel around the ball of the foot and gently pull back.
- Plantar fascia stretch: Pull the toes back gently toward the shin to stretch the sole of the foot.
- Toe curls and marble pick-ups: These help strengthen the small muscles of the foot.
- Resistance-based foot exercises: Useful for gradually improving foot control and tolerance.
The key here is consistency rather than heroics. Gentle daily work usually beats doing one epic stretch session and then limping about feeling virtuous.
Orthotic Insoles and Supportive Footwear
Footwear matters more than many people realise. NICE-backed guidance recommends comfortable shoes with good support, and the wider evidence base continues to support orthoses as part of management for plantar heel pain. :contentReference[oaicite:5]{index=5}
Wearing supportive shoes and using insoles for plantar fasciitis can help reduce repeated strain on the fascia throughout the day. A well-designed insole may cushion impact, support the arch and improve pressure distribution under the heel and forefoot.
Orthotic insoles can be over-the-counter or custom. Over-the-counter options are often a sensible first step for common heel pain. Custom devices may be more appropriate where there are clear biomechanical issues, persistent symptoms or complex foot structure concerns.
Helpful footwear features for plantar fasciitis: a stable heel, decent cushioning, removable insoles, good arch support, and enough room in the toe box without the shoe feeling sloppy.
Night Splints for Morning Heel Pain
Night splints are commonly recommended when pain is worst with the first steps in the morning. They hold the ankle in a dorsiflexed position overnight, which keeps the plantar fascia and Achilles tendon on a gentle stretch. The logic is simple: if the tissue tightens overnight, the first few steps can feel brutal; keeping it slightly lengthened may reduce that morning shock. This approach appears in both clinical guidance and supporting evidence reviews.
Night splints are often most useful in chronic or stubborn cases, especially where morning pain is a standout feature. They are not always glamorous, and some people need a short adjustment period, but they can be a very useful part of the overall treatment mix.
Physical Therapy and Manual Techniques
Physical therapy can be helpful when symptoms are not settling or when you need a more tailored plan. A therapist may work on calf flexibility, ankle mobility, foot strength and loading strategy, while also helping you progress activity safely.
Manual techniques such as massage, soft tissue work and mobilisation are often used alongside exercise. At home, simple tools like a massage ball or a chilled bottle rolled under the arch can help calm the area down temporarily, especially after long days on your feet.
Lifestyle Changes and Load Management
Plantar fasciitis recovery is not just about what you add. It is also about what you reduce. If your feet are taking a hammering every day, the fascia has very little chance to settle down. Load management matters.
- Reduce prolonged standing where possible during flare-ups
- Swap high-impact exercise temporarily for lower-impact options
- Avoid walking barefoot on hard floors if that aggravates symptoms
- Rotate shoes rather than relying on one flattened-out pair every day
- Consider weight management if excess load is a factor
Supportive shoes, adjusted activity and sensible pacing are repeatedly highlighted in UK guidance and evidence summaries.
Shockwave Therapy for Chronic Plantar Fasciitis
When symptoms persist despite good conservative care, extracorporeal shockwave therapy may be considered. This treatment uses sound waves to stimulate the painful area and is most often discussed for chronic plantar heel pain rather than early, mild cases. Best-practice evidence includes shockwave therapy among options that may be used in a structured care pathway for more persistent symptoms.
Shockwave therapy is non-invasive, but it is not usually the first thing tried. It makes more sense after footwear, orthoses, stretching and load-management basics have had a fair run.
Injections and Other Advanced Treatments
For cases that do not improve, clinicians may discuss more advanced options such as injections or other interventional treatments. These decisions depend on symptom duration, examination findings and whether other causes of heel pain have been ruled out. They are usually considered only after conservative care has been used properly and consistently. Evidence summaries on plantar heel pain include injections among later-stage options, but they are not the starting point for most people.
PRP is still being explored in the literature and may be offered in some settings, but it is better described as an emerging or selective option rather than a universal standard treatment. That keeps the article strong without overselling it.
Surgery for Severe or Persistent Cases
Surgery is typically reserved for the minority of cases that remain severe and persistent after extended conservative treatment. It is generally treated as a last resort because recovery can be lengthy and surgery always carries risk. Most people improve without needing to go anywhere near an operating theatre, which is encouraging both for patients and for anyone not especially keen on foot surgery as a hobby.
How Long Does Plantar Fasciitis Take to Heal?
There is no single magic timetable. Some people improve within weeks, while others need several months, especially if symptoms have been present for a long time or the aggravating factors are still ongoing. Evidence-led guidance supports patience and consistency with conservative care, particularly stretching, footwear, orthoses and load management.
The important point is this: plantar fasciitis often responds to steady, boring, sensible treatment. That may not be exciting, but it is usually more effective than bouncing randomly between gadgets, miracle cures and internet folklore.
Frequently Asked Questions
How long does plantar fasciitis usually last?
It varies. Some cases improve within 6 to 12 weeks, while others can take several months, especially if the foot continues to be overloaded or the condition has been present for a long time.
Can plantar fasciitis go away on its own?
Mild cases can ease with rest and better footwear, but symptoms usually settle faster and more reliably with stretching, support and a proper treatment plan.
Are insoles worth trying for plantar fasciitis?
Yes, for many people they are. Supportive insoles can reduce strain on the plantar fascia and improve comfort during walking and standing.
Are night splints actually helpful?
They can be, particularly if morning pain is one of your main symptoms. They work best as part of a wider plan rather than as the only treatment.
Should I stop exercise completely?
Usually not. It is more about modifying activity than stopping everything. Lower-impact exercise is often a better short-term option while symptoms settle.
Are high heels bad for plantar fasciitis?
For many people, yes. Unsupportive footwear or shoes that change how load is distributed through the foot can aggravate symptoms. Stable, supportive shoes are usually a better choice.
Final Thoughts
Plantar fasciitis is common, frustrating and sometimes stubborn, but it is also very manageable in most cases. The most effective approach usually combines stretching, supportive shoes, orthotic insoles, activity adjustment and patience. If symptoms are lingering, a podiatrist or physiotherapist can help guide the next step, whether that means night splints, physical therapy, shockwave treatment or a more tailored recovery plan.













Sold: Pair
Incl. VAT Exl. VAT