



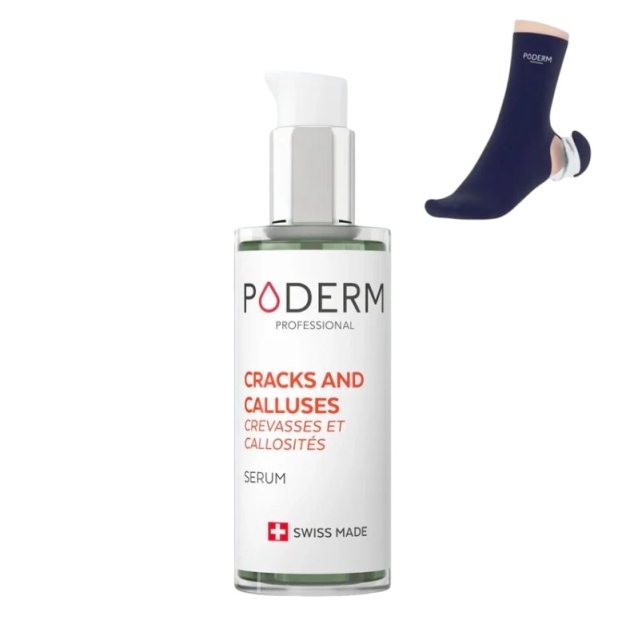
Corns and calluses remain among the most frequent foot complaints in primary care and podiatry. This updated guide for 2025 summarises definitions, current evidence, stepwise care, and when to consider surgical referral for persistent lesions.
Definition
Corn - a localised hyperkeratotic focus with a firm central keratin core that develops from sustained pressure. Often painful on direct pressure and typically over bony prominences or between toes in the case of soft corns.
Callus - a broader plaque of diffuse hyperkeratosis due to friction or shear. Usually less tender than a corn and often over weight bearing areas.
Both are adaptive responses to mechanical stress. Removing or redistributing the offending force allows the skin to return toward a softer and more pliable state.
Key sources: NHS • PCDS
How it works and why it matters
Repetitive pressure and shear stimulate keratinocyte proliferation and thickening of the stratum corneum. The focal hard plug of a corn can press on cutaneous nerves which causes sharp pain on direct load. Untreated lesions can split or ulcerate in at risk feet such as those with diabetes or peripheral arterial disease. See DermNet
Modern management emphasises pressure optimisation alongside skilled debridement. UK guidance consistently advises footwear review, protective padding, keratolytics for suitable patients, and referral when deformity or recalcitrance persists. See NHS • Royal College of Podiatry
What users say
“Routine debridement plus a simple toe sleeve changed my day to day comfort. I went from avoiding long walks to enjoying them again.”
“Swapping to wider shoes and using a hydrocolloid plaster gave near instant relief while I waited for my podiatry appointment.”
Patients value pain relief that is quick and practical. Education about footwear fit and pressure redistribution is crucial to prevent cycles of recurrence. See RCPod
Step-by-step guide
1. Assess
- History - site, footwear, activity, occupation, duration, recurrence
- Inspection - hard focal nucleus suggests a corn, diffuse plaque suggests callus
- Differentiate from plantar warts - warts are more tender with squeeze than with direct pressure and often show thrombosed capillaries after paring
- Screen vascular supply and sensation in at risk feet
Differentials and assessment aids: PCDS • Cornwall NHS referral criteria
2. First line conservative care
- Skilled debridement to reduce thickness and pain
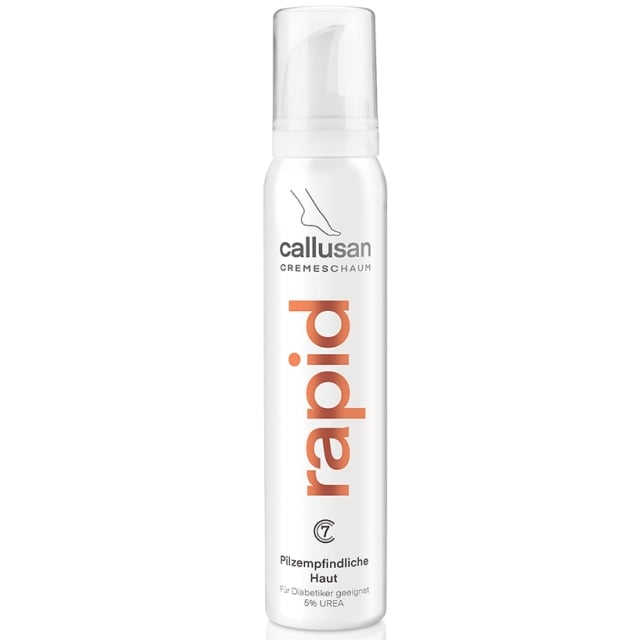
- Daily emollients such as urea based moisturisers ideally under occlusion at night
- Footwear optimisation - wide toe box and soft uppers and avoid seams over pressure points
Self treatment with blades is unsafe for those with diabetes or impaired circulation. NHS
3. Pressure redistribution
- Silicone toe protectors and orthodigital splints for interdigital soft corns
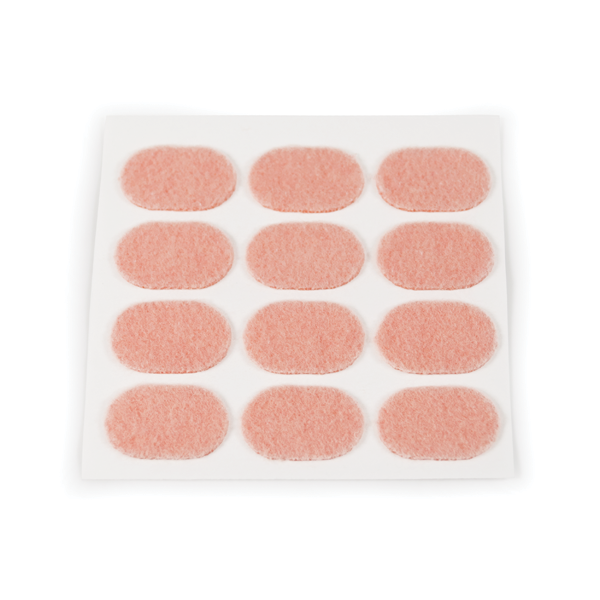
- Felt or foam pads to offload focal metatarsal heads
- Prefabricated or custom insoles to spread load for plantar calluses
Padding and appliances reduce pressure and protect skin. RCPod
4. Keratolytics
- Salicylic acid preparations - plasters, paints, gels used with care
- Urea or lactic acid creams for regular softening
- Avoid keratolytics on broken skin and avoid in at risk feet unless advised by a clinician
Licensing and strengths vary. Bazuka Extra Strength gel 26% salicylic acid is licensed in the UK for warts verrucae corns and calluses. NICE CKS - topical salicylic acid
5. Review and maintain
- Reassess lesion size tenderness and footwear fit
- Repeat conservative debridement as required
- Reinforce self care and emollient adherence
6. When to escalate
- Recurrent painful lesions that persist despite optimal offloading
- Underlying deformity such as hammer toe or exostosis
- Consider imaging and surgical opinion for structural correction
Metatarsal osteotomy or digital procedures can be effective when carefully planned to avoid transfer lesions. See referral guidance: Cornwall NHS
Evidence note - a pragmatic UK trial comparing 40% salicylic acid plasters with usual scalpel enucleation demonstrated favourable clinical and economic outcomes for plasters in many patients. Appropriate selection and monitoring are key. J Foot Ankle Res • NIHR summary
Comparison tables
Approaches to management
| Domain | Conservative | Adjunctive | Surgical |
|---|---|---|---|
| Typical interventions | Debridement and emollients and footwear optimisation and pads and orthoses | Hydrocolloid plasters and targeted keratolytics and silicone sleeves | Digital correction and exostectomy and metatarsal osteotomy and forefoot realignment |
| Invasiveness | Low | Low to moderate | High |
| Risks | Minor skin irritation if over pared | Local irritation and maceration if occluded for too long | Infection and wound issues and transfer lesions if malaligned |
| Recurrence control | Moderate if pressure is controlled | Moderate to high when combined with offloading | Variable and dependent on biomechanical success |
| Best suited for | Most first presentations and low grade lesions | Refractory lesions without major deformity | Recurrent lesions with correctable deformity |
Orthotic and padding options
| Device | Use case | Pros | Watch outs |
|---|---|---|---|
| Silicone orthodigital splints | Soft corns between toes | Easy to mould and washable and cushioning | Ensure correct size to avoid maceration |
| Felt or foam pads | Focal metatarsal head overload | Immediate offloading and low cost | Can shift pressure if poorly positioned |
| Prefabricated insoles | Diffuse forefoot callus | Accessible and can be trialled quickly | May not fully resolve heavy callus build up |
| Custom insoles | Persistent symptoms with specific biomechanical drivers | Tailored redistribution and durable | Requires expert fitting and review |
| Hydrocolloid plasters | Painful focal corns and calluses | Cushioning and hydration and discreet | Do not use on broken skin |
FAQ
Can I pare a corn at home
Not with a blade. Gentle use of a foot file on intact skin is acceptable for some but at risk patients such as those with diabetes or impaired circulation should avoid self treatment and seek professional care. NHS guidance
Which creams are best
Urea based moisturisers help soften thickened skin. Keratolytics such as salicylic acid can be effective when used as directed on intact skin. Strength and formulation matter and pharmacist or clinician advice is recommended. NICE CKS
Do orthoses really help
Yes for many people. Insoles and pads redistribute pressure that drives hyperkeratosis. Relief can be significant although complete prevention of callus build up is not guaranteed. Royal College of Podiatry
When should I see a specialist
Seek assessment if pain persists despite footwear changes and padding and emollients. Immediate review is advised if there is bleeding or ulceration or significant deformity or recurrent breakdown. Referral criteria example
Are salicylic acid plasters better than scalpel enucleation
Both can relieve symptoms. A UK trial suggested that 40% salicylic acid plasters can be at least as effective as usual scalpel care for many patients with potential cost advantages. Selection and monitoring are important. J Foot Ankle Res
How do I find an NHS podiatry service
Use the NHS services finder to locate podiatrists and chiropodists in your area. NHS Service Search
Case vignette - excision of an intractable corn
A 63 year old male presented with a long standing painful corn under the right forefoot. Conservative care including repeated debridement and pads gave only transient relief. Surgical excision revealed a 1.5 cm epithelial lined cyst within dense fibrosis beneath the hyperkeratosis. The lesion was excised and postoperative offloading provided. Symptoms resolved fully without recurrence at review. This highlights the need to consider subdermal pathology or bony prominence when pain persists despite meticulous conservative care.
Soft tissue pain and associated conditions
Persistent hyperkeratosis can coexist with bursitis and capsulitis and tendinopathy caused by repetitive overload. Conservative management remains first line - load management and footwear change and orthoses and physiotherapy. Severe tendon injuries or rigid deformities may need surgical correction to restore function and reduce pathologic pressure.
Conclusion
Effective care for corns and calluses rests on three pillars - reduce the mechanical cause and normalise the skin and prevent recurrence. That means footwear that fits and thoughtful padding and orthoses combined with skilled debridement and targeted keratolytics for appropriate patients. When structural deformity or subdermal pathology sustains the lesion and conservative measures fail a surgical opinion is reasonable. Early attention to pressure can prevent chronic tissue change and maintain comfort and mobility.
References and research sources
- NHS. Corns and calluses. Page reviewed 24 August 2022 and next review due 24 August 2025. https://www.nhs.uk/conditions/corns-and-calluses/
- Royal College of Podiatry. Corns and callus. https://rcpod.org.uk/common-foot-problems/corns-callus
- Primary Care Dermatology Society. Corns and callosities - clinical guidance. https://www.pcds.org.uk/clinical-guidance/callosities-and-corns
- Vlahovic TC et al. The effectiveness of salicylic acid plasters compared with usual scalpel treatment for corns. J Foot Ankle Res. 2013. https://jfootankleres.biomedcentral.com/articles/10.1186/1757-1146-6-40
- NIHR. The long term effectiveness of 40% salicylic acid plasters on corns - award summary. https://fundingawards.nihr.ac.uk/award/PB-PG-0807-14060
- NICE CKS. Topical salicylic acid - UK prescribing information. https://cks.nice.org.uk/topics/warts-verrucae/prescribing-information/topical-salicylic-acid/
- DermNet. Corns and calluses. https://dermnetnz.org/topics/corn-callus
- Cornwall NHS. Corns and calluses - referral criteria and differential pointers. https://rms.cornwall.nhs.uk/.../corns_and_calluses
- NHS services search - find podiatrists and chiropodists. https://www.nhs.uk/service-search/other-health-services/podiatrists-and-chiropodists
Links tested 16 October 2025.
Author
Marc Cameron - Algeos
Marc Cameron is a producr specialist with experience in lower limb biomechanics and conservative foot care. He focuses on practical guidance that blends evidence with real world clinic workflow.














Sold: Each
Incl. VAT Exl. VAT