





Pressure Relieving Insoles - How do they help people with Diabetes?
For people living with diabetes, the right in-shoe pressure management can be the difference between staying active and developing a preventable foot ulcer. Pressure-relieving diabetic insoles are a practical clinical tool that reduces harmful plantar loading and helps protect high-risk tissue.
Definition
- Pressure relieving Diabetic Insoles
- In-shoe inserts designed to redistribute plantar pressure away from vulnerable areas, reduce peak pressure, and improve comfort and stability during walking and standing.
- Who they are for
- Most commonly used for people with diabetes at risk of skin breakdown due to neuropathy, deformity, previous ulceration, or elevated plantar pressure.
- What they are not
- They are not a substitute for urgent assessment of a hot swollen foot, a new wound, signs of infection, or sudden skin colour change.
DIabetic Insoles: How they work - biomechanics in plain terms
Diabetes-related peripheral neuropathy can reduce protective sensation, so a person may not notice rubbing, blistering or minor trauma. When that loss of sensation combines with repeated high pressure under the forefoot or heel, skin and soft tissue can break down over time.
Pressure-relieving insoles address this by changing how load is applied through the sole of the foot.
1) Redistribute pressure away from hot spots
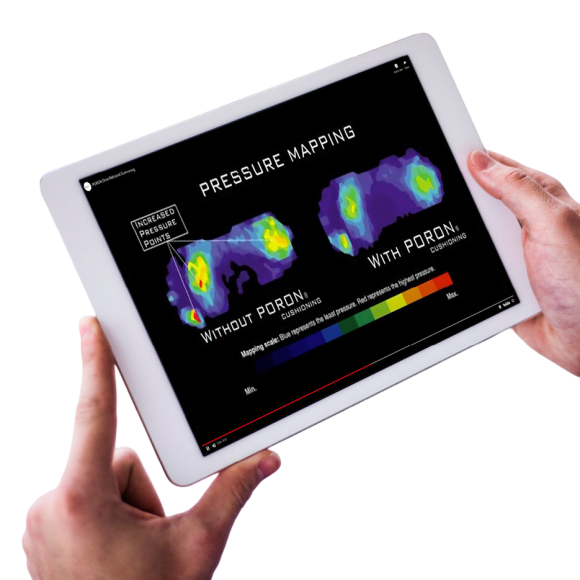
Many diabetic ulcers start at predictable high-load points such as metatarsal heads or the hallux. A well-selected insole increases contact area and shifts load away from peak-pressure zones. International guidance emphasises prescribing therapeutic footwear that demonstrates a pressure-relieving effect during walking for prevention of recurrent plantar ulcers. IWGDF guidance on footwear and offloading
2) Cushion impact and reduce shear stress
Soft top covers and resilient bases dampen impact forces. Some designs also help reduce shear forces. These sliding forces can be as damaging as vertical pressure. This is especially true for calluses and thin plantar fat pads.
3) Improve fit and reduce internal rubbing
Therapeutic footwear guidance from NHS services commonly describes shock-absorbing insoles that support feet evenly and reduce abnormal pressure to the soles. Fit matters because volume, seam placement, and insole interface can cause rubbing that a neuropathic foot may not feel. NHS patient leaflet on therapeutic footwear
Why it matters
Diabetic foot disease is preventable in many cases with early risk identification, regular foot checks, and timely offloading. UK guidance focuses on structured care pathways and foot protection services for people at risk. NICE NG19: Diabetic foot problems - prevention and management
Key benefits for people with diabetes
- Lower ulcer risk: Reducing peak plantar pressure helps protect tissue that is repeatedly overloaded.
- Support for ulcer remission: After an ulcer heals, pressure relief and high wear-time are central to reducing recurrence risk.
- Comfort and confidence: Better shock absorption and support can make walking feel safer and less fatiguing.
- Encourages adherence: Comfortable insoles are more likely to be worn at home and outdoors, which matters because wear-time is protective.
Risks and limitations to manage
- False reassurance: An insole does not replace daily skin inspection and rapid escalation for red flags.
- Poor fit can worsen pressure: If the insole crowds the toe box it can increase dorsal pressure on toes or nails.
- Material fatigue: Cushioning compresses over time so the pressure profile can drift and require review.
NHS patient information on foot ulcers highlights the importance of wearing special footwear or insoles as advised to help prevent further ulcers. NHS England foot ulcer information guide
Insole approaches in diabetes
| Option | Best for | Strengths | Watch-outs |
|---|---|---|---|
| Soft accommodative insoles | Neuropathy with sensitive feet, mild deformity, early prevention | Comfort, cushioning, improved contact area | May compress sooner, needs review and replacement |
| Multi-density pressure relief | Higher plantar pressures, callus, metatarsal head overload | Targeted offloading while maintaining stability | Needs correct footwear volume and trimming |
| Custom orthoses with pressure mapping | Previous ulcer, significant deformity, recurrent focal pressure | Most precise redistribution when well made and well fitted | Cost, lead time, requires clinical review and patient adherence |
| Integrated offloading devices | Active ulcer healing where stronger offloading is needed | Guidelines support higher level offloading for healing | May require specialist fitting and monitoring |

What users say
While experiences vary by foot shape and shoe choice, feedback tends to cluster into a few practical themes:
- Comfort changes behaviour: People often report they walk more confidently when pressure points feel calmer.
- Reduced callus build-up: Some notice less hard skin under metatarsal heads when pressure is better distributed.
- Better tolerance of long days: Cushioning can reduce end-of-day soreness, especially for people who stand at work.
- Adherence is the challenge: The most common barrier is not the insole itself, it is wearing appropriate footwear consistently, including at home.
Step-by-step guide - selecting and using diabetic insoles safely
Step 1: Stratify risk
Identify neuropathy, previous ulcer, deformity, callus, peripheral arterial disease, or Charcot risk. Use your local pathway aligned with national guidance. NICE NG19
Step 2: Choose the right footwear first
- Check width and depth, especially toe box height.
- Look for minimal internal seams and a stable heel counter.
- Ensure the insole lies flat with no curling edges.
NHS therapeutic footwear information describes shock-absorbing insoles designed to support feet evenly and reduce abnormal pressure. NHS therapeutic footwear leaflet
Step 3: Select the insole category
For low to moderate risk, a quality accommodative insole may be sufficient. For previous ulceration or clear focal overload, consider a higher level solution and referral for customisation and pressure assessment. International guidance supports prescribing footwear with a demonstrated pressure-relieving effect for recurrent ulcer prevention. IWGDF guidance (Wiley PDF)
Step 4: Fit, trim, and check
- Trim precisely to the shoe last, not the old insole if it is distorted.
- Confirm there is no rocking and no raised edges.
- Ask the person to stand and walk, then re-check toe space and heel seating.
Step 5: Break-in plan and skin surveillance
- Start with 1-2 hours on day one and build gradually over a week if risk is moderate and skin is intact.
- Daily inspection of plantar skin, toes, and heel is essential, using a mirror if needed.
- Escalate urgently if there is a new red area that does not blanch, any break in skin, swelling, heat, or discharge.
Step 6: Review schedule
Review fit and wear patterns at 4-6 weeks, then at least every 3-6 months for high-risk patients. Replace when compression set or top cover wear changes the interface, or sooner if the foot status changes.
FAQ
1) Do pressure-relieving insoles prevent diabetic foot ulcers?
They can reduce risk by lowering peak plantar pressure and improving load distribution, especially when combined with appropriate footwear and consistent wear. For people with prior plantar ulcers, international guidance recommends therapeutic footwear with a demonstrated pressure-relieving effect during walking. IWGDF guidance
2) Are over-the-counter insoles enough?
Sometimes, for lower-risk feet with intact skin and minimal deformity. If there is neuropathy, deformity, heavy callus, or previous ulceration, a higher level assessment is often appropriate. NICE NG19
3) Should insoles be worn at home?
Yes if advised. Patient information from NHS services commonly stresses wearing prescribed footwear or insoles as much as possible to help prevent further ulcers. NHS England guide
4) How do I know if an insole is causing problems?
Warning signs include new redness that persists, blisters, hot spots, increased callus, toe rubbing, or nail pressure. Stop use and seek podiatry review promptly if any skin change appears.
5) How often should diabetic insoles be replaced?
It depends on materials, body weight, activity, and shoe use. As a rule, replace when cushioning compresses or the top cover wears through, and reassess more frequently in high-risk feet.
6) Are insoles the same as offloading for an active ulcer?
Not always. Active ulcer healing may require more intensive offloading interventions guided by specialist services and international recommendations. IWGDF Offloading Guideline (2023)
References and research sources
- NICE. Diabetic foot problems: prevention and management (NG19).
- IWGDF. Offloading guideline (2023 update).
- Bus SA et al (IWGDF). Guidance on footwear and offloading interventions to prevent and heal foot ulcers in diabetes.
- NHS England. Diabetes - Foot Ulcers: an information guide (PDF).
- Sheffield Teaching Hospitals NHS Foundation Trust. Therapeutic footwear for diabetic patients (PDF).
- Algeos. Duosoft Therapeutic Diabetic Insoles.
Sold: Sold per Pair
Incl. VAT Exl. VAT